Bursitis Of The Foot Inflammation
Overview
Heel bursitis is also known as retrocalcaneal bursitis. The heel bone is called calcaneus, and the bursa associated with the heel bone is located in the area between the Achilles tendon and calf muscles. When this particular bursa gets aggravated due to constant pressure in the ankle, the posterior end of the heel or the area behind the heel gets inflamed and hence the result is retrocalcaneal bursitis. Strain to the ankles could be caused due to various reasons like extraneous jogging, skipping, or such physical activities that increase the pressure on the ankles.
Causes
Inflammation of the calcaneal bursae is most commonly caused by repetitive overuse and cumulative trauma, as seen in runners wearing tight-fitting shoes. Such bursitis may also be associated with conditions such as gout, rheumatoid arthritis, and seronegative spondyloarthropathies. In some cases, subtendinous calcaneal bursitis is caused by bursal impingement between the Achilles tendon and an excessively prominent posterior superior aspect of a calcaneus that has been affected by Haglund deformity. With Haglund disease, impingement occurs during ankle dorsiflexion.
Symptoms
Achiness or stiffness in the affected joint. Worse pain when you press on or move the joint. A joint that looks red and swollen (especially when the bursae in the knee or elbow are affected). A joint that feels warm to the touch, compared to the unaffected joint, which could be a sign that you have an infection in the bursa. A ?squishy? feeling when you touch the affected part. Symptoms that rapidly reappear after an injury or sharp blow to the affected area.
Diagnosis
Magnetic resonance imaging (MRI) may demonstrate bursal inflammation, but this modality probably does not offer much more information than that found by careful physical examination. Theoretically, MRI could help the physician to determine whether the inflammation is within the subcutaneous bursa, the subtendinous bursa, or even within the tendon itself, however, such testing is generally not necessary. Ultrasonography may be a potentially useful tool for diagnosing pathologies of the Achilles tendon.
Non Surgical Treatment
Physiotherapy treatment is vital to hasten the healing process, ensure an optimal outcome and reduce the likelihood of injury recurrence in all patients with retrocalcaneal bursitis. Treatment may comprise soft tissue massage (particularly to the calf muscles), joint mobilization (of the ankle, subtalar joint and foot), dry needling, electrotherapy (e.g. ultrasound), stretches, the use of heel wedges, the use of crutches, ice or heat treatment, arch support taping, the use of a compression bandage, exercises to improve strength, flexibility, balance and core stability, education, anti-inflammatory advice, activity modification advice, biomechanical correction (e.g. the use of orthotics), footwear advice, a gradual return to activity program.
Surgical Treatment
Only if non-surgical attempts at treatment fail, will it make sense to consider surgery. Surgery for retrocalcanel bursitis can include many different procedures. Some of these include removal of the bursa, removing any excess bone at the back of the heel (calcaneal exostectomy), and occasionally detachment and re-attachment of the Achilles tendon. If the foot structure and shape of the heel bone is a primary cause of the bursitis, surgery to re-align the heel bone (calcaneal osteotomy) may be considered. Regardless of which exact surgery is planned, the goal is always to decrease pain and correct the deformity. The idea is to get you back to the activities that you really enjoy. Your foot and ankle surgeon will determine the exact surgical procedure that is most likely to correct the problem in your case. But if you have to have surgery, you can work together to develop a plan that will help assure success.
Heel bursitis is also known as retrocalcaneal bursitis. The heel bone is called calcaneus, and the bursa associated with the heel bone is located in the area between the Achilles tendon and calf muscles. When this particular bursa gets aggravated due to constant pressure in the ankle, the posterior end of the heel or the area behind the heel gets inflamed and hence the result is retrocalcaneal bursitis. Strain to the ankles could be caused due to various reasons like extraneous jogging, skipping, or such physical activities that increase the pressure on the ankles.
Causes
Inflammation of the calcaneal bursae is most commonly caused by repetitive overuse and cumulative trauma, as seen in runners wearing tight-fitting shoes. Such bursitis may also be associated with conditions such as gout, rheumatoid arthritis, and seronegative spondyloarthropathies. In some cases, subtendinous calcaneal bursitis is caused by bursal impingement between the Achilles tendon and an excessively prominent posterior superior aspect of a calcaneus that has been affected by Haglund deformity. With Haglund disease, impingement occurs during ankle dorsiflexion.
Symptoms
Achiness or stiffness in the affected joint. Worse pain when you press on or move the joint. A joint that looks red and swollen (especially when the bursae in the knee or elbow are affected). A joint that feels warm to the touch, compared to the unaffected joint, which could be a sign that you have an infection in the bursa. A ?squishy? feeling when you touch the affected part. Symptoms that rapidly reappear after an injury or sharp blow to the affected area.
Diagnosis
Magnetic resonance imaging (MRI) may demonstrate bursal inflammation, but this modality probably does not offer much more information than that found by careful physical examination. Theoretically, MRI could help the physician to determine whether the inflammation is within the subcutaneous bursa, the subtendinous bursa, or even within the tendon itself, however, such testing is generally not necessary. Ultrasonography may be a potentially useful tool for diagnosing pathologies of the Achilles tendon.
Non Surgical Treatment
Physiotherapy treatment is vital to hasten the healing process, ensure an optimal outcome and reduce the likelihood of injury recurrence in all patients with retrocalcaneal bursitis. Treatment may comprise soft tissue massage (particularly to the calf muscles), joint mobilization (of the ankle, subtalar joint and foot), dry needling, electrotherapy (e.g. ultrasound), stretches, the use of heel wedges, the use of crutches, ice or heat treatment, arch support taping, the use of a compression bandage, exercises to improve strength, flexibility, balance and core stability, education, anti-inflammatory advice, activity modification advice, biomechanical correction (e.g. the use of orthotics), footwear advice, a gradual return to activity program.
Surgical Treatment
Only if non-surgical attempts at treatment fail, will it make sense to consider surgery. Surgery for retrocalcanel bursitis can include many different procedures. Some of these include removal of the bursa, removing any excess bone at the back of the heel (calcaneal exostectomy), and occasionally detachment and re-attachment of the Achilles tendon. If the foot structure and shape of the heel bone is a primary cause of the bursitis, surgery to re-align the heel bone (calcaneal osteotomy) may be considered. Regardless of which exact surgery is planned, the goal is always to decrease pain and correct the deformity. The idea is to get you back to the activities that you really enjoy. Your foot and ankle surgeon will determine the exact surgical procedure that is most likely to correct the problem in your case. But if you have to have surgery, you can work together to develop a plan that will help assure success.
Hammertoes Treatment
 Overview
Overview
Hammer toes can occur when feet are crammed into shoes so tight that the front of the toes are pushed against the front of the shoes for prolonged periods of time. One or Hammer toe more toes then remain bent with the middle knuckle pointing up, even when shoes are taken off. If the condition is left untreated and tight footwear is continually worn, these bent toes can become so rigid that they can no longer straighten out on their own. While any shoes that are too tight can lead to this condition, high heels seem to be a big culprit since the elevated ankle causes more weight to push the toes forward. This may explain why the condition affects more women than men.
Causes
Many people develop hammertoe because they wear shoes that are too tight. Shoes with narrow toe boxes squeeze the toes together, forcing some to bend. This causes the toe muscles to contract. If the toes are forced into this cramped position too often, the muscles may permanently tighten, preventing the toes from extending. Chronic hammertoe can also cause the long bones that connect the toes to the foot, called metatarsals, to move out of position. The misaligned metatarsal bones may pinch a nerve running between them, which can cause a type of nerve irritation called a neuroma.
 Symptoms
Symptoms
Common symptoms of hammertoes include pain or irritation of the affected toe when wearing shoes. corns and calluses (a buildup of skin) on the toe, between two toes, or on the ball of the foot. Corns are caused by constant friction against the shoe. They may be soft or hard, depending upon their location. Inflammation, redness, or a burning sensation. Contracture of the toe. In more severe cases of hammertoe, open sores may form.
Diagnosis
Your doctor is very likely to be able to diagnose your hammertoe simply by examining your foot. Even before that, he or she will probably ask about your family and personal medical history and evaluate your gait as you walk and the types of shoes you wear. You'll be asked about your symptoms, when they started and when they occur. You may also be asked to flex your toe so that your doctor can get an idea of your range of motion. He or she may order x-rays in order to better define your deformity.
Non Surgical Treatment
What will a doctor do? Treat any foot complaints such as corns, calluses by periodically reducing the lesion and applying appropriate pads and dressings. Recommend the silicone toe prop. If an infection is present, then anti-septic dressings, antibiotics and pads to redistribute pressure away from the lesion may be necessary. In the case of a mallet toe, trigger toe or claw toe. If a corn occurs at the end of the toe, a silicone or leather prop may be used to straighten the toe. In a hammertoe deformity, a silicone prop to redistribute pressure away from a corn may be necessary. The doctor may give footwear advice. In severe cases, corrective surgery may be necessary. The doctor may recommend orthosis to correct a mechanical complaint of the foot, such as 3/4 length silicone insoles.
Surgical Treatment
Surgery may be the treatment of choice if conservative approaches prove unsuccessful. Usually performed as an outpatient procedure, the specific surgery will depend on the type and extent of injury to the toe. Recovery my take several days or weeks and you may experience some redness, stiffness and swelling of the affected toe. Your physician will recommend taking it easy and to keep your foot elevated while you recover.
 Prevention
Prevention
Although these following preventative tips may be able to reverse a painful bunion or hammertoe deformity, they are more effective when applied to young people, and are less effective the longer a person has progressed with their bunion or hammertoe deformity. This is because the joints in our bodies get used to the positions they are most frequently held in, and our feet are no different, with our 12 to 15 hours a day in restrictive footwear, with tapering toeboxes, heel elevation, and toespring.
Hammer Toes Causes Symptoms
 Overview
Overview
A Hammer toes or contracted toe is a deformity of the proximal interphalangeal joint of the second, third, or fourth toe causing it to be permanently bent, resembling a hammer. Mallet toe is a similar condition affecting the distal interphalangeal joint.
Causes
Hereditary and shoe gear are probably the most likely reasons to develop a hammer toe. Tight pointy shoes may cause a hammer hammertoes toes. High heels also can cause hammer toes. A deformed toe often develops over time, and certain types of feet may be predisposed. Some patients may develop a hammer toe or cross over toe (of the 2nd toe) due to a bunion of the big toe.
 Symptoms
Symptoms
A toe (usually the second digit, next to the big toe) bent at the middle joint and clenched into a painful, clawlike position. As the toe points downward, the middle joint may protrude upward. A toe with an end joint that curls under itself. Painful calluses or corns. Redness or a painful corn on top of the bent joint or at the tip of the affected toe, because of persistent rubbing against shoes Pain in the toes that interferes with walking, jogging, dancing, and other normal activities, possibly leading to gait changes.
Diagnosis
Your healthcare provider will examine your foot, checking for redness, swelling, corns, and calluses. Your provider will also measure the flexibility of your toes and test how much feeling you have in your toes. You may have blood tests to check for arthritis, diabetes, and infection.
Non Surgical Treatment
In many cases, conservative treatment consisting of physical therapy and new shoes with soft, spacious toe boxes is enough to resolve the condition, while in more severe or longstanding cases podiatric surgery may be necessary to correct the deformity. The patient's doctor may also prescribe some toe exercises that can be done at home to stretch and strengthen the muscles. For example, the individual can gently stretch the toes manually, or use the toes to pick things up off the floor. While watching television or reading, one can put a towel flat under the feet and use the toes to crumple it. The doctor can also prescribe a brace that pushes down on the toes to force them to stretch out their muscles.
Surgical Treatment
If your hammer, claw, or mallet toe gets worse, or if nonsurgical treatment does not help your pain, you may think about surgery. The type of surgery you choose depends on how severe your condition is and whether the toe joint is fixed (has no movement) or flexible (has some movement). A fixed toe joint often requires surgery to be straightened. A flexible toe joint can sometimes be straightened without surgery. Surgery choices include Phalangeal head resection (arthroplasty), in which the surgeon removes part of the toe bone. Joint fusion (arthrodesis), in which the surgeon removes part of the joint, letting the toe bones grow together (fuse). Cutting supporting tissue or moving tendons in the toe joint. How well surgery works depends on what type of surgery you have, how experienced your surgeon is, and how badly your toes are affected.
 Prevention
Prevention
Hammertoe can usually be prevented by wearing shoes that fit properly and give the toes plenty of room. Don?t wear shoes with pointed or narrow toes. Don?t wear shoes that are too tight or short. Don?t wear high-heeled shoes, which can force the toes forward. Choose shoes with wide or boxy toes. Choose shoes that are a half-inch longer than your longest toe. If shoes hurt, don?t wear them.
What Causes Over-Pronation Of The Foot
Overview
Overpronation is a term used to describe excessive flattening of the plantar arch. Pronation is a normal part of our gait (the way we walk), and it comprises three movements: dorsiflexion, eversion, and abduction. Dorsiflexion is the upward movement of the foot, eversion describes the foot rolling in, and abduction is ?out toeing,? meaning your toes are moving away from the midline of your body. When these three motions are extreme or excessive, overpronation results. Overpronation is very common in people who have flexible flat feet. Flatfoot, or pes planus, is a condition that causes collapse of the arch during weight bearing. This flattening puts stress on the plantar fascia and the bones of the foot, resulting in pain and further breakdown.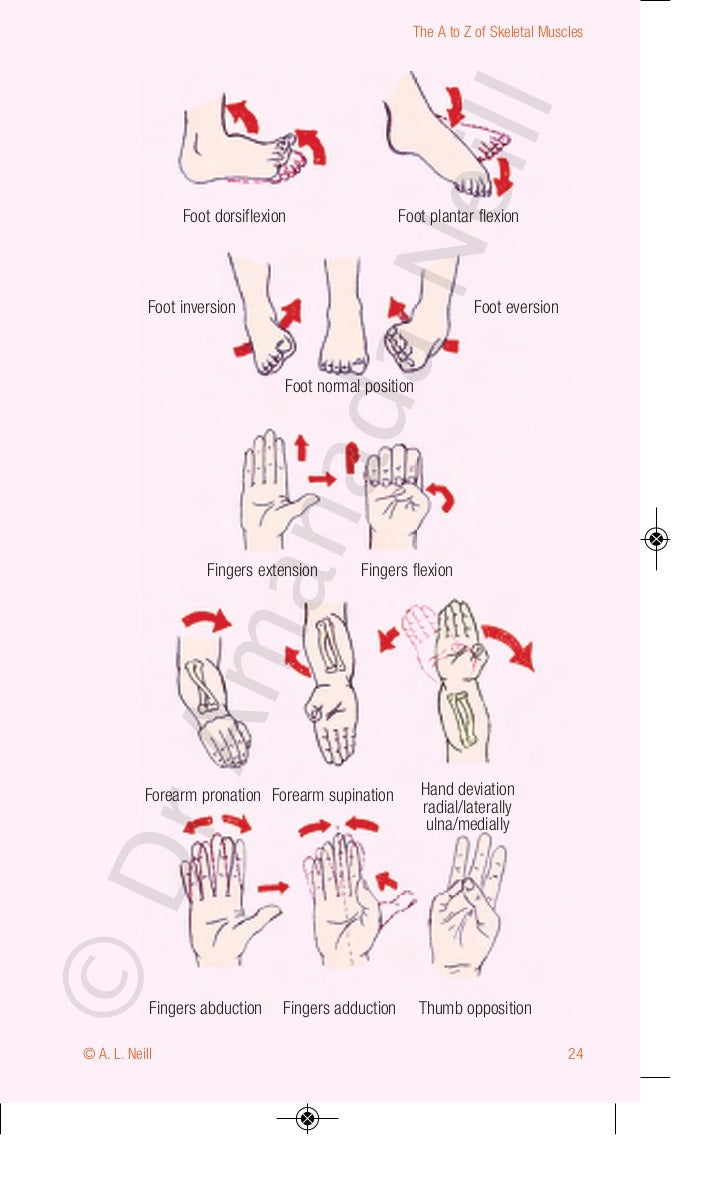
Causes
Flat feet don't automatically mean you have a problem. The problem can be divided into a flexible flat foot or rigid flat foot. The rigid flat foot is one that does not change shape when the foot becomes weight bearing. i.e. it does not go through the excessive motion of pronation. Generally speaking this foot does not provide too many problems. The flexible flat foot is the type that when it becomes weight bearing the foot and ankle tends to roll in (pronates) too far. This type of person will often say I have great arches but when I stand up much of this arch disappears as the foot excessively pronates When the foot is excessively pronating and causing problems like sore ankles, feet or knees when standing or exercising then arch support is extremely important to restore the foot structure.
Symptoms
Common conditions seen with overpronation include heel pain or plantar fasciitis. Achilles tendonopathy. Hallus Valgus and/or bunions. Patellofemoral pain syndrome. Iliotibial band pain syndrome. Low back pain. Shin splints. Stress fractures in the foot or lower leg.
Diagnosis
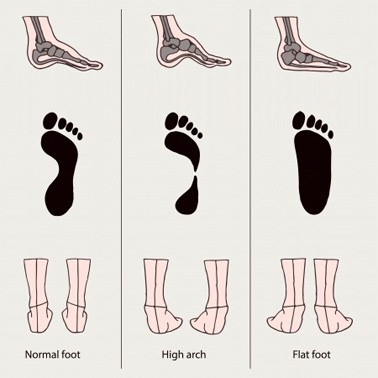
So, how can you tell if you have overpronation, or abnormal motion in your feet, and what plantar fasciitis treatment will work to correct it? Look at your feet. While standing, do you clearly see the arch on the inside of your foot? If not, and if the innermost part of your sole touches the floor, then your feet are overpronated. Look at your (running/walking) shoes. If your shoes are more worn on the inside of the sole in particular, then pronation may be a problem for you. Use the wet foot test. Wet your feet and walk along a section of pavement, then look at the footprints you leave behind. A normal foot will leave a print of the heel connected to the forefoot by a strip approximately half the width of the foot on the outside of the sole. If you?re feet are pronated there may be little distinction between the rear and forefoot.
Non Surgical Treatment
When you see the doctor, he or she will likely perform a complete examination of your feet and watch you walk. The doctor will need to take x-rays to determine the cause of your flat feet. In some cases, further imaging may be needed, especially if your symptoms are severe and sudden in nature. Once you are properly diagnosed, your doctor will create an appropriate treatment plan. There are several options to correct overpronation, such as orthotics. In many cases, overpronation can be treated with non-surgical methods and over-the-counter orthotics. In severe cases, however, custom-made orthotics may work better. Orthotics provide arch support and therefore prevent collapse of the arch with weight bearing. They are made of materials such as spongy rubber or hard plastic. Your doctor will also want to examine your footwear to ensure they fit properly and offer enough medial support. Extra support and stability can be achieved with footwear that has a firm heel counter. If you are experiencing pain, you should be able to use over-the-counter pain medications such as ibuprofen to relieve symptoms.
Prevention
Custom-made orthotics will reduce the twisting of the leg muscles as they enter the foot, by maintaining a normal alignment of the bones and joints of the foot. If the bones and joints are aligned properly, by reducing the pronation, the muscles can run straight to their attachments in the foot, without twisting to get to these bones. This action of custom-made orthotics will reduce Achilles Tendonitis shin splints; ankle, knee, hip, and lower back pain; and leg cramps. This action will also allow the leg muscles to work more efficiently, thus allowing you to walk and run with less effort.
Overpronation is a term used to describe excessive flattening of the plantar arch. Pronation is a normal part of our gait (the way we walk), and it comprises three movements: dorsiflexion, eversion, and abduction. Dorsiflexion is the upward movement of the foot, eversion describes the foot rolling in, and abduction is ?out toeing,? meaning your toes are moving away from the midline of your body. When these three motions are extreme or excessive, overpronation results. Overpronation is very common in people who have flexible flat feet. Flatfoot, or pes planus, is a condition that causes collapse of the arch during weight bearing. This flattening puts stress on the plantar fascia and the bones of the foot, resulting in pain and further breakdown.
Causes
Flat feet don't automatically mean you have a problem. The problem can be divided into a flexible flat foot or rigid flat foot. The rigid flat foot is one that does not change shape when the foot becomes weight bearing. i.e. it does not go through the excessive motion of pronation. Generally speaking this foot does not provide too many problems. The flexible flat foot is the type that when it becomes weight bearing the foot and ankle tends to roll in (pronates) too far. This type of person will often say I have great arches but when I stand up much of this arch disappears as the foot excessively pronates When the foot is excessively pronating and causing problems like sore ankles, feet or knees when standing or exercising then arch support is extremely important to restore the foot structure.
Symptoms
Common conditions seen with overpronation include heel pain or plantar fasciitis. Achilles tendonopathy. Hallus Valgus and/or bunions. Patellofemoral pain syndrome. Iliotibial band pain syndrome. Low back pain. Shin splints. Stress fractures in the foot or lower leg.
Diagnosis
So, how can you tell if you have overpronation, or abnormal motion in your feet, and what plantar fasciitis treatment will work to correct it? Look at your feet. While standing, do you clearly see the arch on the inside of your foot? If not, and if the innermost part of your sole touches the floor, then your feet are overpronated. Look at your (running/walking) shoes. If your shoes are more worn on the inside of the sole in particular, then pronation may be a problem for you. Use the wet foot test. Wet your feet and walk along a section of pavement, then look at the footprints you leave behind. A normal foot will leave a print of the heel connected to the forefoot by a strip approximately half the width of the foot on the outside of the sole. If you?re feet are pronated there may be little distinction between the rear and forefoot.
Non Surgical Treatment
When you see the doctor, he or she will likely perform a complete examination of your feet and watch you walk. The doctor will need to take x-rays to determine the cause of your flat feet. In some cases, further imaging may be needed, especially if your symptoms are severe and sudden in nature. Once you are properly diagnosed, your doctor will create an appropriate treatment plan. There are several options to correct overpronation, such as orthotics. In many cases, overpronation can be treated with non-surgical methods and over-the-counter orthotics. In severe cases, however, custom-made orthotics may work better. Orthotics provide arch support and therefore prevent collapse of the arch with weight bearing. They are made of materials such as spongy rubber or hard plastic. Your doctor will also want to examine your footwear to ensure they fit properly and offer enough medial support. Extra support and stability can be achieved with footwear that has a firm heel counter. If you are experiencing pain, you should be able to use over-the-counter pain medications such as ibuprofen to relieve symptoms.
Prevention
Custom-made orthotics will reduce the twisting of the leg muscles as they enter the foot, by maintaining a normal alignment of the bones and joints of the foot. If the bones and joints are aligned properly, by reducing the pronation, the muscles can run straight to their attachments in the foot, without twisting to get to these bones. This action of custom-made orthotics will reduce Achilles Tendonitis shin splints; ankle, knee, hip, and lower back pain; and leg cramps. This action will also allow the leg muscles to work more efficiently, thus allowing you to walk and run with less effort.
Dealing With Calcaneal Apophysitis
Overview
Sever?s disease, also known as calcaneal apophysitis or Osgood-Schlatter syndrome of the foot. This traction apophysitis is secondary to repetitive microtraumata or overuse of the heel in young athletes. The calcaneus is situated at the most plantar posterior aspect of the foot. The Achilles tendon inserts to the lower, posterior and slightly medial aspect of the calcaneus. The plantar fascia originates from the medial tubercle on the plantar aspect of the calcaneus. Proximal to the epiphysis is the apophysis, where the Achilles tendon actually inserts. The calcaneal growth plate and apophysis are situated in an area subject to high stress from the plantar and Achilles tendon.
Causes
Sever's disease is a common cause of heel pain in physically active growing kids. It usually occurs during the growth spurt of adolescence, the approximately 2-year period in early puberty when kids grow most rapidly. This growth spurt can begin anytime between the ages of 8 to 13 for girls and 10 to 15 for boys. Peak incidences are girls, 8 to 10 years old. boys, 10 to 12 years old.
Symptoms
Sever?s disease is a clinical diagnosis based on the youth?s presenting symptoms, rather than on diagnostic tests. While x-rays may be ordered in the process of diagnosing the disease, they are used primarily to rule out bone fractures or other bone abnormalities, rather than to confirm the disease. Common Characteristics of Sever?s Disease include Posterior inferior heel pain. Pain is usually absent when waking in the morning. Increased pain with weight bearing, running, or jumping (or activity-related pain). Area often feels stiff or inflexible. Youth may limp at the end of physical activity. Tenderness at the insertion of the tendons. Limited ankle dorsiflexion range that is secondary to tightness of the Achilles tendon. Activity or sport practices on hard surfaces can also contribute to pain, as well as poor quality shoes, worn out shoes, or the wrong shoes for the sport. Typically, the pain from this disease gradually resolves with rest.
Diagnosis
Children or adolescents who are experiencing pain and discomfort in their feet should be evaluated by a physician. In some cases, no imaging tests are needed to diagnose Sever?s disease. A podiatrist or other healthcare professional may choose to order an x-ray or imaging study, however, to ensure that there is no other cause for the pain, such as a fracture. Sever?s disease will not show any findings on an x-ray because it affects cartilage.
Non Surgical Treatment
A physiotherapist will assess your pain, presentation and biomechanics. They can then treat your sever?s disease with hands on techniques which may include massage, manual therapy and taping. Your physiotherapist can then provide advice on what you can do at home to further progress your treatment, this may include stretching, strengthening and activity modification. In some cases orthotic prescription may be of benefit.
Prevention
Perform a well rounded dynamic warm up before activity. Perform a good static stretching routine after activity. Increase core strength. Perform exercises that emphasize active lengthening of the calf muscles. Use proper footwear. Avoid excessive running or jumping on hard surfaces like concrete by using better surfaces such as asphalt, gymnasium floors or grass.
Sever?s disease, also known as calcaneal apophysitis or Osgood-Schlatter syndrome of the foot. This traction apophysitis is secondary to repetitive microtraumata or overuse of the heel in young athletes. The calcaneus is situated at the most plantar posterior aspect of the foot. The Achilles tendon inserts to the lower, posterior and slightly medial aspect of the calcaneus. The plantar fascia originates from the medial tubercle on the plantar aspect of the calcaneus. Proximal to the epiphysis is the apophysis, where the Achilles tendon actually inserts. The calcaneal growth plate and apophysis are situated in an area subject to high stress from the plantar and Achilles tendon.
Causes
Sever's disease is a common cause of heel pain in physically active growing kids. It usually occurs during the growth spurt of adolescence, the approximately 2-year period in early puberty when kids grow most rapidly. This growth spurt can begin anytime between the ages of 8 to 13 for girls and 10 to 15 for boys. Peak incidences are girls, 8 to 10 years old. boys, 10 to 12 years old.
Symptoms
Sever?s disease is a clinical diagnosis based on the youth?s presenting symptoms, rather than on diagnostic tests. While x-rays may be ordered in the process of diagnosing the disease, they are used primarily to rule out bone fractures or other bone abnormalities, rather than to confirm the disease. Common Characteristics of Sever?s Disease include Posterior inferior heel pain. Pain is usually absent when waking in the morning. Increased pain with weight bearing, running, or jumping (or activity-related pain). Area often feels stiff or inflexible. Youth may limp at the end of physical activity. Tenderness at the insertion of the tendons. Limited ankle dorsiflexion range that is secondary to tightness of the Achilles tendon. Activity or sport practices on hard surfaces can also contribute to pain, as well as poor quality shoes, worn out shoes, or the wrong shoes for the sport. Typically, the pain from this disease gradually resolves with rest.
Diagnosis
Children or adolescents who are experiencing pain and discomfort in their feet should be evaluated by a physician. In some cases, no imaging tests are needed to diagnose Sever?s disease. A podiatrist or other healthcare professional may choose to order an x-ray or imaging study, however, to ensure that there is no other cause for the pain, such as a fracture. Sever?s disease will not show any findings on an x-ray because it affects cartilage.
Non Surgical Treatment
A physiotherapist will assess your pain, presentation and biomechanics. They can then treat your sever?s disease with hands on techniques which may include massage, manual therapy and taping. Your physiotherapist can then provide advice on what you can do at home to further progress your treatment, this may include stretching, strengthening and activity modification. In some cases orthotic prescription may be of benefit.
Prevention
Perform a well rounded dynamic warm up before activity. Perform a good static stretching routine after activity. Increase core strength. Perform exercises that emphasize active lengthening of the calf muscles. Use proper footwear. Avoid excessive running or jumping on hard surfaces like concrete by using better surfaces such as asphalt, gymnasium floors or grass.
The Treatments And Causes
Overview
Becoming flatfooted can be a real health issue for people. The advice from healthcare experts is to pay attention to foot pain, and when it happens, to seek help right away. In the last 20 years, adult-acquired flatfoot has become a more commonly recognized health issue. The cause is a dysfunction of the ankle tendon that attaches to the bones on the inside of your foot. The function of this posterior tibial tendon (PTT) is to maintain the foot arch and provide strength during push-off when you walk. When the PTT is not functioning correctly, you tend to lose your arch, or become more flatfooted. This problem occurs about three times more often in women than in men, especially after the age of 40. Initially, PTT dysfunction is associated with pain on the inside of the ankle, swelling and sometimes a limp. If left unchecked, the arch appears to collapse and the pain on the inside of the ankle worsens. Eventually, if left unchecked, patients will begin to feel pain on the outside of the ankle, too. 
Causes
There are numerous causes of acquired Adult Flatfoot, including, trauma, fracture, dislocation, tendon rupture/partial rupture or inflammation of the tendons, tarsal coalition, arthritis, neuroarthropathy and neurologic weakness. The most common cause of acquired Adult Flatfoot is due to overuse of a tendon on the inside of the ankle called the posterior tibial tendon. This is classed as - posterior tibial tendon dysfunction. What are the causes of Adult Acquired flat foot? Trauma, Fracture or dislocation. Tendon rupture, partial tear or inflammation. Tarsal Coalition. Arthritis. Neuroarthropathy. Neurological weakness.
Symptoms
Some symptoms of adult acquired flat foot are pain along the inside of the foot and ankle, pain that increases with activity, and difficulty walking for long periods of time. You may experience difficulty standing, pain on the outside of the ankle, and bony bumps on the top of the foot and inside the foot. You may also have numbness and tingling of the feet and toes (may result from large bone spurs putting pressure on nerves), swelling, a large bump on the sole of the foot and/or an ulcer (in diabetic patients). Diabetic patients should wear a properly fitting diabetic shoe wear to prevent these complications from happening.
Diagnosis
Although you can do the "wet test" at home, a thorough examination by a doctor will be needed to identify why the flatfoot developed. Possible causes include a congenital abnormality, a bone fracture or dislocation, a torn or stretched tendon, arthritis or neurologic weakness. For example, an inability to rise up on your toes while standing on the affected foot may indicate damage to the posterior tibial tendon (PTT), which supports the heel and forms the arch. If "too many toes" show on the outside of your foot when the doctor views you from the rear, your shinbone (tibia) may be sliding off the anklebone (talus), another indicator of damage to the PTT. Be sure to wear your regular shoes to the examination. An irregular wear pattern on the bottom of the shoe is another indicator of acquired adult flatfoot. Your physician may request X-rays to see how the bones of your feet are aligned. Muscle and tendon strength are tested by asking you to move the foot while the doctor holds it.
Non surgical Treatment
PTTD is a progressive condition. Early treatment is needed to prevent relentless progression to a more advanced disease which can lead to more problems for that affected foot. In general, the treatments include rest. Reducing or even stopping activities that worsen the pain is the initial step. Switching to low-impact exercise such as cycling, elliptical trainers, or swimming is helpful. These activities do not put a large impact load on the foot. Ice. Apply cold packs on the most painful area of the posterior tibial tendon frequently to keep down the swelling. Placing ice over the tendon immediately after completing an exercise helps to decrease the inflammation around the tendon. Nonsteroidal Anti-inflammatory Medication (NSAIDS). Drugs, such as arcoxia, voltaren and celebrex help to reduce pain and inflammation. Taking such medications prior to an exercise activity helps to limit inflammation around the tendon. However, long term use of these drugs can be harmful to you with side effects including peptic ulcer disease and renal impairment or failure. Casting. A short leg cast or walking boot may be used for 6 to 8 weeks in the acutely painful foot. This allows the tendon to rest and the swelling to go down. However, a cast causes the other muscles of the leg to atrophy (decrease in strength) and thus is only used if no other conservative treatment works. Most people can be helped with orthotics and braces. An orthotic is a shoe insert. It is the most common non-surgical treatment for a flatfoot and it is very safe to use. A custom orthotic is required in patients who have moderate to severe changes in the shape of the foot. Physiotherapy helps to strengthen the injured tendon and it can help patients with mild to moderate disease of the posterior tibial tendon. 
Surgical Treatment
A new type of surgery has been developed in which surgeons can re-construct the flat foot deformity and also the deltoid ligament using a tendon called the peroneus longus. A person is able to function fully without use of the peroneus longus but they can also be taken from deceased donors if needed. The new surgery was performed on four men and one woman. An improved alignment of the ankle was still evident nine years later, and all had good mobility 8 to 10 years after the surgery. None had developed arthritis.
Arch Pain Triggers Warning Signs And Treatments
Overview
Flat feet are characterized by no arch in the inner foot. It can be a genetic condition or the result of improper body mechanics. Often the whole of the foot will contact the ground. A healthy foot structure supports the body's weight from the bone structure arch; a flat foot is unable to properly support this weight, causing pressure in the ankle, knee and hip joints.

Causes
Conditions that affect the nervous system (brain and spinal cord) can also cause the arches to fall. Over time, the muscles gradually become stiffer and weaker and lose their flexibility. Conditions where this can occur include cerebral palsy, spina bifida and muscular dystrophy. Adult-acquired flat feet often affect women over 40 years of age. It often goes undiagnosed and develops when the tendon that supports the foot arch gradually stretches over time. It's not fully understood what causes the tendon to become stretched, but some experts believe that wearing high heels and standing or walking for long periods may play a part. Obesity, high blood pressure (hypertension) and diabetes are all risk factors.
Symptoms
If you've ever seen your footprints in the sand and they looked more like bricks than feet, then you probably have flat feet. Simply stated, a flat foot is a foot that does not have an arch when standing. In the medical world, flat feet are associated with "pronated" feet. Pronated is merely the term used to describe the position of the foot when it is flexed upward (dorsiflexed), turned away from the body (abducted), and the heel is rolled outward (everted), all at the same time. A certain amount of pronation is required for normal walking, but too much pronation is often considered a foot's "worst enemy." Over time, excessive pronation can lead to many unpleasant problems including heel pain, bunions, hammertoes, shin splints, and even knee, hip, or back pain. In fact, one orthopedic surgeon discovered that 95% of his total knee replacement patients and 90% of his total hip replacement patients had flat feet. An easy way to tell if you pronate too much is to take a look at your athletic shoes-excessive wearing of the inside heel (arch side of the shoe) as compared to the outside is a classic indication of excessive pronation.
Diagnosis
A professional therapist may use tinels test to diagnose tarsal tunnel syndrome. This involves tapping the nerve just behind the medial malleolus or bony bit of the ankle with a rubber hammer. Pain indicates a positive test. Sometimes it is initially mistaken for plantar fasciitis which also causes pain from the inside heel and throughout the arch of the foot. Neural symptoms (such as tingling or numbness) as well as the location of tenderness when touching the area should help to easily distinguish between the conditions.
Non Surgical Treatment
Treatment of plantar fasciitis is sometimes a drawn out and frustrating process. A program of rehabilitation should be undertaken with the help of someone qualified and knowledgeable about the affliction. Typically, plantar fasciitis will require at least six weeks and up to six months of conservative care to be fully remedied. Should such efforts not provide relief to the athlete, more aggressive measures including surgery may be considered. The initial goals of physical therapy should be to increase the passive flexion of the foot and improve flexibility in the foot and ankle, eventually leading to a full return to normal function. Prolonged inactivity in vigorous sports is often the price to be paid for thorough recovery. Half measures can lead to a chronic condition, in some cases severely limiting athletic ability.
Surgical Treatment
With flat feet, there is a tendon on the inside of the foot than can often become weakened, injured, split and/or ruptured. This tendon, is called the posterior tibial tendon, and is the main arch supporting tendon. Obviously damage to this tendon can cause collapse of the arch. Some people have genetically inefficient tendon, and tends to be the case in younger people. In mild cases, such as tendon splits, the posterior tibial tendon can be repaired to restore its strength. Acute incontinuity of the tendon can be primarily repaired. Often the posterior tibial tendon is augmented with a tendon transfer of an adjacent tendon to provide both strength and continuity. In any tendon repair, advanced or retensioning of the tendon is performed. In most flat foot surgery a tendon augmentation is often combined with other boney procedures to restore structure and balance to the foot.
Stretching Exercises
You may start exercising the muscles of your foot right away by gently stretching and strengthening them. Frozen can roll. Roll your bare injured foot back and forth from your heel to your mid-arch over a frozen juice can. Repeat for 3 to 5 minutes. This exercise is particularly helpful if it is done first thing in the morning. Towel stretch. Sit on a hard surface with your injured leg stretched out in front of you. Loop a towel around your toes and the ball of your foot and pull the towel toward your body keeping your leg straight. Hold this position for 15 to 30 seconds and then relax. Repeat 3 times. Standing calf stretch. Stand facing a wall with your hands on the wall at about eye level. Keep your injured leg back with your heel on the floor. Keep the other leg forward with the knee bent. Turn your back foot slightly inward (as if you were pigeon-toed). Slowly lean into the wall until you feel a stretch in the back of your calf. Hold the stretch for 15 to 30 seconds. Return to the starting position. Repeat 3 times. Do this exercise several times each day. Seated plantar fascia stretch. Sit in a chair and cross the injured foot over the knee of your other leg. Place your fingers over the base of your toes and pull them back toward your shin until you feel a comfortable stretch in the arch of your foot. Hold 15 seconds and repeat 3 times. Plantar fascia massage. Sit in a chair and cross the injured foot over the knee of your other leg. Place your fingers over the base of the toes of your injured foot and pull your toes toward your shin until you feel a stretch in the arch of your foot. With your other hand, massage the bottom of your foot, moving from the heel toward your toes. Do this for 3 to 5 minutes. Start gently. Press harder on the bottom of your foot as you become able to tolerate more pressure.
Flat feet are characterized by no arch in the inner foot. It can be a genetic condition or the result of improper body mechanics. Often the whole of the foot will contact the ground. A healthy foot structure supports the body's weight from the bone structure arch; a flat foot is unable to properly support this weight, causing pressure in the ankle, knee and hip joints.
Causes
Conditions that affect the nervous system (brain and spinal cord) can also cause the arches to fall. Over time, the muscles gradually become stiffer and weaker and lose their flexibility. Conditions where this can occur include cerebral palsy, spina bifida and muscular dystrophy. Adult-acquired flat feet often affect women over 40 years of age. It often goes undiagnosed and develops when the tendon that supports the foot arch gradually stretches over time. It's not fully understood what causes the tendon to become stretched, but some experts believe that wearing high heels and standing or walking for long periods may play a part. Obesity, high blood pressure (hypertension) and diabetes are all risk factors.
Symptoms
If you've ever seen your footprints in the sand and they looked more like bricks than feet, then you probably have flat feet. Simply stated, a flat foot is a foot that does not have an arch when standing. In the medical world, flat feet are associated with "pronated" feet. Pronated is merely the term used to describe the position of the foot when it is flexed upward (dorsiflexed), turned away from the body (abducted), and the heel is rolled outward (everted), all at the same time. A certain amount of pronation is required for normal walking, but too much pronation is often considered a foot's "worst enemy." Over time, excessive pronation can lead to many unpleasant problems including heel pain, bunions, hammertoes, shin splints, and even knee, hip, or back pain. In fact, one orthopedic surgeon discovered that 95% of his total knee replacement patients and 90% of his total hip replacement patients had flat feet. An easy way to tell if you pronate too much is to take a look at your athletic shoes-excessive wearing of the inside heel (arch side of the shoe) as compared to the outside is a classic indication of excessive pronation.
Diagnosis
A professional therapist may use tinels test to diagnose tarsal tunnel syndrome. This involves tapping the nerve just behind the medial malleolus or bony bit of the ankle with a rubber hammer. Pain indicates a positive test. Sometimes it is initially mistaken for plantar fasciitis which also causes pain from the inside heel and throughout the arch of the foot. Neural symptoms (such as tingling or numbness) as well as the location of tenderness when touching the area should help to easily distinguish between the conditions.
Non Surgical Treatment
Treatment of plantar fasciitis is sometimes a drawn out and frustrating process. A program of rehabilitation should be undertaken with the help of someone qualified and knowledgeable about the affliction. Typically, plantar fasciitis will require at least six weeks and up to six months of conservative care to be fully remedied. Should such efforts not provide relief to the athlete, more aggressive measures including surgery may be considered. The initial goals of physical therapy should be to increase the passive flexion of the foot and improve flexibility in the foot and ankle, eventually leading to a full return to normal function. Prolonged inactivity in vigorous sports is often the price to be paid for thorough recovery. Half measures can lead to a chronic condition, in some cases severely limiting athletic ability.
Surgical Treatment
With flat feet, there is a tendon on the inside of the foot than can often become weakened, injured, split and/or ruptured. This tendon, is called the posterior tibial tendon, and is the main arch supporting tendon. Obviously damage to this tendon can cause collapse of the arch. Some people have genetically inefficient tendon, and tends to be the case in younger people. In mild cases, such as tendon splits, the posterior tibial tendon can be repaired to restore its strength. Acute incontinuity of the tendon can be primarily repaired. Often the posterior tibial tendon is augmented with a tendon transfer of an adjacent tendon to provide both strength and continuity. In any tendon repair, advanced or retensioning of the tendon is performed. In most flat foot surgery a tendon augmentation is often combined with other boney procedures to restore structure and balance to the foot.
Stretching Exercises
You may start exercising the muscles of your foot right away by gently stretching and strengthening them. Frozen can roll. Roll your bare injured foot back and forth from your heel to your mid-arch over a frozen juice can. Repeat for 3 to 5 minutes. This exercise is particularly helpful if it is done first thing in the morning. Towel stretch. Sit on a hard surface with your injured leg stretched out in front of you. Loop a towel around your toes and the ball of your foot and pull the towel toward your body keeping your leg straight. Hold this position for 15 to 30 seconds and then relax. Repeat 3 times. Standing calf stretch. Stand facing a wall with your hands on the wall at about eye level. Keep your injured leg back with your heel on the floor. Keep the other leg forward with the knee bent. Turn your back foot slightly inward (as if you were pigeon-toed). Slowly lean into the wall until you feel a stretch in the back of your calf. Hold the stretch for 15 to 30 seconds. Return to the starting position. Repeat 3 times. Do this exercise several times each day. Seated plantar fascia stretch. Sit in a chair and cross the injured foot over the knee of your other leg. Place your fingers over the base of your toes and pull them back toward your shin until you feel a comfortable stretch in the arch of your foot. Hold 15 seconds and repeat 3 times. Plantar fascia massage. Sit in a chair and cross the injured foot over the knee of your other leg. Place your fingers over the base of the toes of your injured foot and pull your toes toward your shin until you feel a stretch in the arch of your foot. With your other hand, massage the bottom of your foot, moving from the heel toward your toes. Do this for 3 to 5 minutes. Start gently. Press harder on the bottom of your foot as you become able to tolerate more pressure.